



 Publications
Publications
 Partners
Partners




There are reasons to be cautiously optimistic about South Africa's prospects of surviving the Covid-19 pandemic.
To understand this, we must consider what countries that have fared well have in common, and the same for countries that have fared badly.
Below is a table setting out the death rate in countries prominent in the drama, from the worst to the best, together with possible relevant factors that could make a difference.
As a sample, I chose most of the countries that have been prominent in the news lately for their role in dealing with the virus, either badly or well.
I deliberately left out China, because it is under a cloud relating to data and it operated in a different time frame to most other countries to some extent.
There are very patchy statistics on lockdowns and similar measures on a country-by-country basis and for the moment, I am ignoring that.
There is a difference between a lockdown and international travel, which I consider to some extent in the shape of international tourist arrivals on a per capita, per annum basis.
As a primary measure of success or failure, I make use of mortality per million people of each country's population, rather than the much-disputed mortality rate as a percentage of confirmed cases. The latter is, to some extent, a function of the number of tests carried out. I return to that topic later.
The statistics are as at 7 April 2020.

The first point to make is that one of the best markers of high mortality is a cold climate.
In the table, the top quadrant are all European countries from the northern part of the continent, except for Italy and Spain. Major differences are, however, hidden in the various regions of both countries. Italy is especially striking in this regard.
No less than 92.5% of its fatalities occurred in the northern part of Italy, namely north of the 44ºN latitude. To visualise this, 44ºN is the line where the top of the "boot" disappears into the broader continent. The northern regions, we must remember, are bordered mostly by Austria and Switzerland, and much of it forms part of the Alps. The remaining plus-minus 75% to the south is responsible for only 7.5% of deaths.
Similar remarks apply to Spain. About 66% of all fatalities in Spain come from the portion of the country from Madrid northwards. Snow is quite common in Spain, especially in the Pyrenees and in other mountainous areas, like Sierra Nevada, and is not limited to the mountainous areas either.
One of the mysteries puzzling me in dealing with this topic, has been Greece. Freely drawing on my biases, at first blush I saw Greece as the perfect candidate for the pandemic to spread: a stereotypical example of a laid-back Mediterranean country with little discipline when it comes to financial regulations (ask Angela Merkel) and (more to the point) health and travel directives. Not to mention a pumping tourist trade and much extended family accommodation. It should have been flat on its back by now.
Yet it turns out that Greece boasts a very modest 8 per million Covid-19 mortality rate. Why is that?
Looking at the map, and remembering images of sun-baked Greek beach resorts, I then noticed that Greece lies almost entirely south of the 40ºN latitude – on a par with the toe of Italy's boot, if you will. Its temperature, as shown in the table, averages 15.4ºC (Italy 13.45). But contrary to Italy, that average does not mask vast differences in regional temperatures. Greece is in fact, as the brochures boast, mild, warm and often hot. But not really cold.
If we turn to the bottom quartile in the table – the relatively successful survivors of the pandemic so far – we find that the hot countries there too, have very few fatalities.
Notably, Singapore and Hong Kong have sub-tropical climates, and very low fatalities from the virus. Indeed, there is not a single tropical or sub-tropical country in the world with a high mortality figure. India (not in the table) stands at 0.1 deaths per million. It is reasonable to expect that, like seasonal influenza, the novel coronavirus flourishes in the cold, and that by contrast, a warm environment cramps its style.
It further stands to reason that countries with busy travel, especially from countries regarded as hotspots, where the virus was prevalent, would pose a danger. To examine this, I use tourism statistics, namely the number of annual tourists per capita.
Both Spain and Italy have high tourism numbers. In fact, all the countries in the first quartile have more than one tourist per year for every inhabitant (or expressed as a percentage, 100%), with the exception of the UK, which itself stands at an above-average 50%.
By contrast, in the fourth quartile, all the countries have relatively low tourism numbers, with the exception of Hong Kong, which is the territory in the entire table with the highest percentage of tourists per capita by far. As argued earlier, it is most probably protected by its balmy tropical climate. Anyone familiar with the wonderful, crowded, bustling bastion of freedom that Hong Kong is, will appreciate what a risk it would have run, unless it had something more than travel bans and attempts at social distancing to protect it.
However, that is not the end of the matter. One of the outstanding features of the story of the pandemic has been the low mortality figures of the former East bloc countries. In the table, I did not bother to list them all, but they have, without exception, very low fatality rates due to Covid-19. I found that puzzling. Although these countries all fall in the cold part of Europe and they have, for the most part, very healthy and growing tourist industries, they seem to have bucked the trend.
That is where the number of hospital beds per capita enters the picture. It is clear from the table above that countries with high numbers of beds per capita, correlate with low mortality. That is hardly surprising. Hospital beds, of course, in turn, correlate with infrastructure that supports each bed, including ventilators and other ICU equipment. Here is a graphic showing the shortages in some countries.
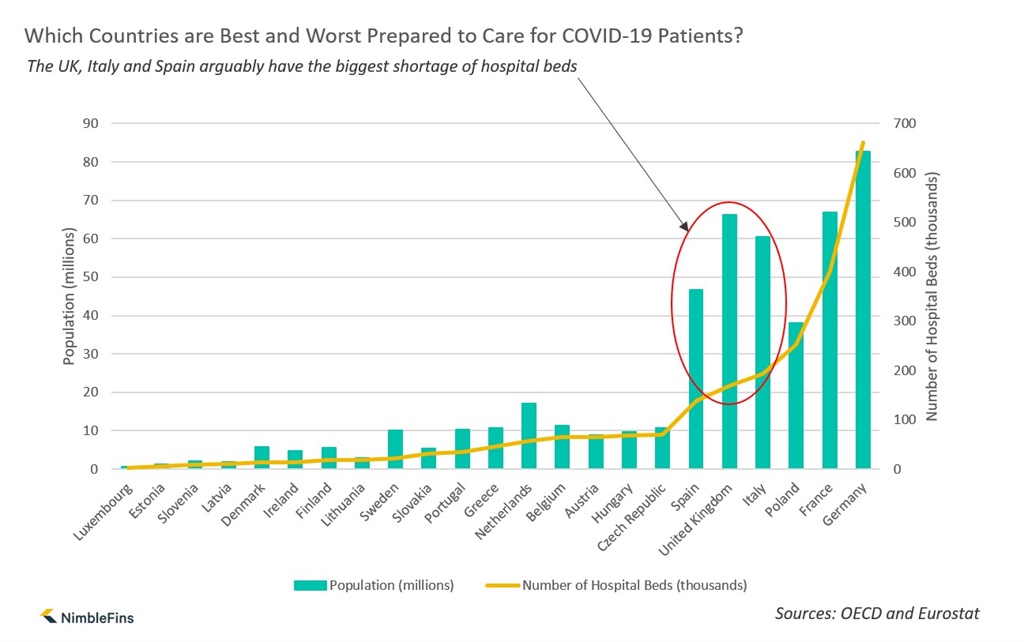
It cannot escape attention that Italy and Spain, the two problem children, have a relative shortage of beds. Worryingly too, so does the UK.
Even more significant is the number of beds per person over the age of 70, as global Covid-19 fatalities fall almost exclusively in that demographic. These numbers are absolutely dominated by countries such as Hungary (54.9 beds per person over 70), Poland (60.5), Slovak Republic (59.2) and Lithuania (46.5). By contrast, Spain has 21.1, Italy 19.1 and the UK 19.5.
It is not feasible to make a similar age-based comparison for South Africa, as the percentage of people over the age of 70 is small, life expectancy being 64 compared to European countries, where it is typically over 75. As for the general population, South Africa has 2.8 beds per 1 000 persons, which is at the low end of the spectrum. Obviously this is a red flag.
As for testing, we have been told that it is crucial to a campaign to fight Covid-19. The numbers do not seem to bear that out, however. Japan and Poland, both relatively successful, have very low testing numbers. Japan has almost ignored testing as a preventative measure. Switzerland and Italy, both less successful, have sky-high testing numbers.
Which does not mean that testing is irrelevant. Targeted testing of high-risk groups (old people, returning travellers, those in contact with infected patients and so on) may enable a country to quarantine or isolate infected persons earlier. Who is tested, may be more important than how many.
Testing is significant for another reason. It is fair to accept that the higher the percentage of people tested in a country, the more that signifies a wide-ranging programme of testing, and less targeting of only sick or high-risk patients. Targeted testing is likely to throw up a higher positive rate of diagnosis, all other things being equal. That means that a country with a low rate of testing and a low positive diagnosis rate, is probably in a good position. An example is Japan, which has a low rate of testing, a low positive diagnosis rate, a low number of cases per million and low mortality. Until recently, Hong Kong and Hungary were in a similar position, but their testing numbers have moved up recently – while their positive diagnosis rates have, significantly, declined.
In a successful country, the more you test, the lower the positive diagnosis rate. Importantly, South Africa shows a lowering rate too. Over the last two weeks before publication of this article, its positive rate declined from 6% to 4%. As presently advised, that rate should decline over time as testing rates increase. South Africa's rate of confirmed cases at this stage (28 per million) is also very low by international standards.
What is also meaningful, is that in countries with low mortality, the infection rate is also low – which in turn, suggests that the virus probably has a slower transmission rate in those territories.
That compels me to revisit the idea of international travel. The success of the ex-East bloc group is clearly not only their high numbers of hospital beds. As the table shows, those countries have had not only low mortality rates, but also low percentages of confirmed cases. That is in spite of customarily high levels of tourist traffic.
It makes sense to exclude foreign carriers of the virus if that is the route by which it reaches the general population. In this regard it is notable that many countries have imposed bans on cross-border entry by travelers especially from "hotspots" where the pandemic has been rife. Examples are the East bloc countries referred to above, Canada (by targeting sick or symptom-bearing entrants, quarantining all foreigners for 14 days and locking the borders to foreign travel, except the US), Japan (to some extent, by banning entry from hotspots like China as early as February) and Russia. On the other hand, the countries in the first quartile were all reasonably slow to impose any form of entry bans.
Despite all the above evidence, there are a few countries that remain outliers. Especially Japan and Russia, that are close to and have trade and travel connections with China, have low infection and mortality rates that seem to be hard to swallow. Can it really be that these countries, both of which are situated in cold regions, both of which are part of global tourism networks, could have escaped almost unscathed?
That brings us to the wild card, which is a recent study that demonstrates a link between countries where BCG vaccination against TB is compulsory, and low mortality due to Covid-19. BCG is the most common vaccination used to prevent TB, but has been associated with successfully fighting other conditions such as leprosy.
I collected the data myself from the BCG Atlas, published by PLOS, and inserted it in the table above. According to the Atlas there are different categories of vaccination. Some countries never had any programme, others used to have an obligatory programme but have terminated it and still others continue to implement it.
From the information summarised in the table, it is clear that the above three categories follow a geographical pattern. Asia, Africa and South America largely have universal vaccination. Most countries in Europe used to have programmes, but have terminated them. North America (the US and Canada) have never had any programmes. The same applies to the Netherlands and significantly, Italy.
The information in the table appears to confirm a correlation between universal vaccination on one hand, and low distribution and mortality on the other.
BCG vaccination as factor would seem to solve some of the mysteries with which I have grappled above: It seems to help explain why the ex-communist countries, including Russia, have displayed not only low mortality, but also low transmission. Your hospitals can be as good as you want, but medical care cannot stop community transmission. The same applies to Japan. BCG might also help explain India's low mortality. China, in the end, has low mortality figures too, although the conventional wisdom is that its success is the result of its rigorous quarantine and lockdown measures. The same applies to South Korea. Perhaps that theory should be revisited in the light of BCG.
That BCG vaccination is not foolproof, if it has any effect, is obvious. That can be ascribed to a number of possible reasons. One is that no programme, especially in the developing world, is likely to be truly universal. Secondly, it is not clear whether the vaccination merely improves resistance, or provides complete immunity. The former seems to be the case.
There are a number of interesting cases to watch, in order to get clarity. In South America there is only one country that has terminated its vaccination programme, and that is Ecuador. Here is the comparison:
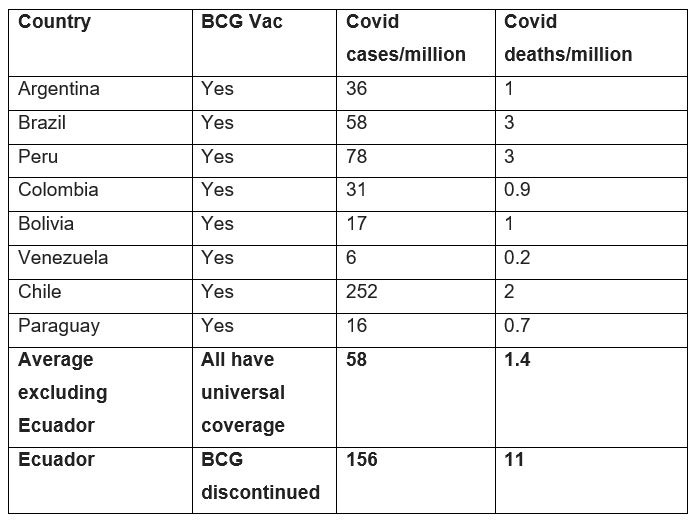
The vaccinated societies in South America are about 3 times as successful on average in terms of cases, and almost 8 times in terms of fatalities, as Ecuador.
Ecuador is important for a different reason. The reason is it has most of the protection factors already identified, including tropical heat and modest tourism traffic.
Although Ecuador seems to be an outlier in the context of South America, in global terms it is a good performer. It would rank with the more successful third quartile in terms of the prominent countries investigated as set out in the table. That again, seems to confirm that relatively low inward travel and a tropical climate still protect to some extent, despite the absence of BCG. BCG does not exclude the effect of the other factors. Their effect appears to be relative to and cumulative with that of BCG.
The relevance of climate is also confirmed by the clear differences between warm and cold regions in Italy, for example.
Where does all that place South Africa?
The first point to make here is that our tourism travel from abroad has been historically low. Ironically, that there have been only 17 tourists per person per year, now looks like a bonus. What is more, as the result of the government's travel ban there are now practically no foreign flights into our country. Leaving aside the impact that that is bound to have on the economy, it would most certainly choke off the influx of carriers from other territories.
The other good news is South Africa's relatively warm climate. Whereas it is true that we are currently heading into winter, our winter is relatively mild compared to that of the north of Italy, and the rest of Europe to the north of that. Indeed, our average temperature is slightly warmer than even that of Greece. Again, one remains mindful of the fact that that average masks considerable differences. Even so, contrary to the Alpine regions of Italy, say, snow is a rare occurrence here.
Here is a list of South Africa's peers in terms of average and coldest-month temperatures, and their records thus far ito deaths from the virus.
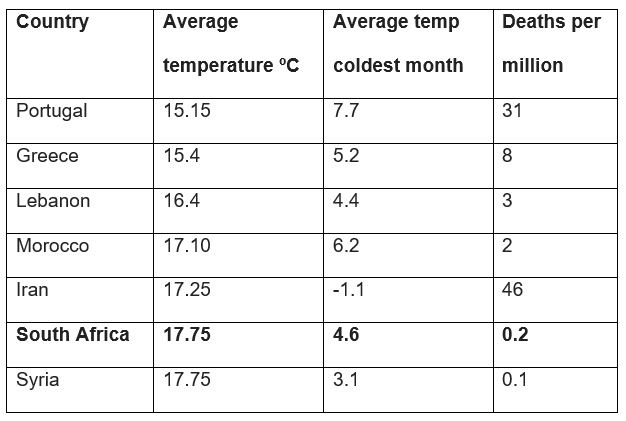
It is notable that Iran, the one with the highest mortality in this peer group, also has a significantly colder winter climate. It is also worth noting that Portugal, with the next highest mortality, has very high tourism arrivals, namely 158% (1.58 tourists per capita per year).
As for BCG, according to the WHO, in 2018 SA had about 70% coverage of BCG immunisation. There are some reports of shortages of the vaccine in recent years, as well as side effects in HIV/Aids patients.
Even so, based on the above evidence, BCG could be a game changer.
There is of course not only good news. With our high incidence of HIV/Aids (273 per 100 000 people) and TB (59 per 100 000) as well as influenza and pneumonia (86 per 100 000), there is no telling how that will interact with the rest of the factors investigated in this article. There is little to compare us to. The load of immuno-suppressing diseases that our population carries, is arguably the heaviest in the world.
But we are not alone. There are countries with immuno-suppressing diseases and conditions that are very severe, notably India with diarrhoeal diseases (40 deaths per 100 000 people), lung disease, including asthma and fibrosis (96 per 100 000), most of North Africa with extremely high rates of influenza (well over 100 per 100 000), West Africa with endemic malaria (50-60 per 100 000) and Mexico with extreme diabetes (88 per 100 000).
Despite these conditions, none of these countries displayed transmission or mortality rates remotely comparing with those in Europe. Here are examples of Covid mortality rates of the most afflicted countries: India 0.1, Chad 0, Nigeria 0.02, DRC 0.2 and Mexico 1 per million people.
Like those countries, South Africa has in its favour the following factors associated with protection against transmission as well as mortality:
- Relatively low tourism travel into the country, (now in SA solidified as a travel ban);
- A warm climate;
- Reasonably wide BCG vaccination coverage.
What we do know is that the horror of the virus "jumping the socio-economic divide" between developed and developing world – in the sense of a surge in infection matching or exceeding problematic rates in Europe - has not happened. It has not happened in India, it has not happened in crisis-ridden Venezuela, and importantly, it has not happened in Africa. Is it so unreasonable to conclude that, for once, the developed world is more at risk of a disease, due to some degree of complacency bred by its own success? It turns out a lack of global travel, third-world medical procedures and - would you know - some global warming, might be a boon.
So, I am cautiously optimistic that we are OK. Medically, that is.
The real fight lies in climbing out of the economic hole we have dug for ourselves, which is a topic for another day.
- Frans Rautenbach is an advocate and labour lawyer at the Cape Town Bar with and the author of South Africa Can Work.


















